New York
ECMO Patient Transport on an Air Ambulance Flight from New York to Mumbai

What is ECMO?
Extracorporeal membrane oxygenation (ECMO) is a life support machine. People who need ECMO have a severe and life-threatening illness that stops their heart or lungs from working properly. For example, ECMO is used during life-threatening conditions such as severe lung damage from infection, or shock after a massive heart attack.
The ECMO machine replaces the function of the heart and lungs. People who need support from an ECMO machine are cared for in a hospital’s intensive care unit (ICU). Typically, people are supported by an ECMO machine for only a few hours to days, but may require it for a few weeks, depending on how their condition progresses. There are many overlaps and differences between the use of ECMO in children and adults. For a focus on Pediatric ECMO, please refer to the Medline Plus resource listed at the end, in addition to this document.
Why is ECMO used?
ECMO is used to help people whose: ■ Lungs cannot provide enough oxygen to the body even when given extra oxygen ■ Lungs cannot get rid of carbon dioxide even with help from a mechanical ventilator ■ Heart cannot pump enough blood to the body ECMO may also be used to support people with heart or lung disease that cannot be cured while they wait for an organ transplant (e.g. new heart and/or lungs).
How does an ECMO machine work?
The ECMO machine is connected to a patient through plastic tubes (cannula). The tubes are placed in large veins and arteries in the legs, neck or chest. The procedure by which a healthcare provider places these tubes in a patient is called cannulation. The ECMO machine pumps blood from the patient’s body to an artificial lung (oxygenator) that adds oxygen to it and removes carbon dioxide. Thus, it replaces the function of the person’s own lungs. The ECMO machine then sends the blood back to the patient via a pump with the same force as the heart, replacing its function. The ECMO machine is controlled by a person called a perfusionist, or a nurse or respiratory therapist with advanced training called an ECMO specialist. The perfusionist or ECMO specialist will adjust the settings on the machine to give the patient the amount of heart and lung support they need.
How is a patient on an ECMO machine monitored?
Any patient connected to an ECMO machine in the ICU is also connected to monitors. These monitors measure heart rate, blood pressure, and oxygen levels. Patients on ECMO need their blood tested very often to measure the oxygen and carbon dioxide levels.
These tests are called blood gases. Patients on ECMO are also given a medication to thin the blood so it does not clot. Thus, the blood is tested frequently to make sure it is thin enough. Members of the patient’s health care team use all these results to see how well the ECMO machine is helping the patient, and to make changes if needed.
How long is an ECMO machine used?
An ECMO machine can help save a patient’s life, but it does not treat the patient’s disease or injury. An ECMO machine simply provides support for a patient while the healthcare team works on treating the underlying disease or injury (such as an infection) or until organs for transplant become available. Healthcare providers will always try to help people get off the ECMO machine as soon as possible. Some diseases or injuries can be treated quickly, and patients only need the ECMO machine for a few hours. Other conditions may take longer to get better, in which case the patient may need the ECMO machine for several days to weeks. Unfortunately, in some cases, patients do not improve enough to be taken off the ECMO machine. ECMO does not save everyone but it has improved survival for many critically ill people who are not responding to usual life support options.
How does it feel to be on ECMO?
When a patient is first being connected to an ECMO machine, he or she is sedated and does not feel the tubes going into their veins and arteries. A person on ECMO is usually already connected to a breathing machine (ventilator) through a tube (endotracheal or ET tube) that is placed in the mouth or nose and down into the windpipe. (For more information, see Mechanical Ventilation at www. thoracic.org/patients). Once connected to an ECMO machine, the cannulae are not painful. Patients who are on an ECMO machine may be given medicines (sedatives or pain controllers) to keep them comfortable. These medicines may also make them sleepy. Other patients are awake and can talk and interact with people while on an ECMO machine. In some cases, patients can exercise to help build up their strength while they are on an ECMO machine. However, some movements can cause the ECMO tubes to get kinked, so patients need to be assisted and carefully supervised when they are moving.
What are the risks of being on ECMO?
The healthcare team looking after patients on ECMO aim to avoid any complications that may occur from being on the machine. Some of the more serious problems that may occur when a patient is on ECMO include: Bleeding: Because of the blood thinning medication that patients need while on ECMO, they can start bleeding in different parts of their body. This can be a very serious problem if the bleeding happens in their brain, lungs, insertion sites of cannulae or from their stomach. The healthcare team monitors patients very carefully by frequent physical exams and lab tests to make sure there is no bleeding. If there is bleeding, then medications can be given to help the blood to clot. Sometimes, surgery is needed to stop the bleeding. Blood and other blood products (such as platelets) may also need to be given if blood counts drop too low. Kidney Failure: Patients who are on ECMO sometimes do not get enough blood flow to their kidneys. This can cause their kidneys to stop working, known as “acute renal failure”. If the kidneys stop working, then a patient may need to be connected to a machine that does the work of the kidneys. This is called dialysis. The kidney damage may get better. However, in some cases, patients may need dialysis for the rest of their life. Infection: The tubes from the ECMO machine go from outside the patient’s body directly into their bloodstream. This increases the risk for infection, because the tubes are a way for germs to enter the body. The infection can reach the lungs, or any other part of the body. Infections in patients on ECMO can usually be treated with antibiotics. However, some patients who develop infections while on ECMO can get sicker and suffer organ damage. Leg Damage: Some patients are connected to the ECMO machine through a vein or artery in their thigh. In some cases, this can impair the blood flow down that leg, and the tissue in the leg can die. If this happens, doctors will try to get blood flowing back down the leg. This usually means changing the ECMO tubing to another part of the body. Unfortunately, the damage can occasionally be bad enough that the patient needs surgery to correct the problem, which may include amputation (removal of part of the leg). Stroke: In patients on ECMO, certain areas of the brain may not get as much blood flow as they need because of small blood clots. This can cause a stroke, and parts of the brain may be permanently damaged. The area of the brain that is damaged will determine what problems a person has from a stroke. Some patients may not be able to move certain parts of their body, see, remember, speak, read or write. Sometimes a person will recover some function after a stroke, but that is not always the case. Fortunately, strokes are very rare and happen less than 5% of the time to patients on ECMO.
How does a patient get taken off ECMO?
The ECMO machine supports the patient while he or she tries to overcome a disease or injury. If the disease or injury improves, the patient may not need the support of the ECMO machine anymore. The healthcare providers will slowly reduce the amount of support the ECMO machine is providing to see if the patient will be okay without it, just like they do with a ventilator (See ATS Patient Education Document on Mechanical Ventilation). If the patient remains stable (or improves) as this is being done, the ECMO tubes are removed and surgeons stitch the entry spots up to close them.
What happens if a patient cannot be taken off ECMO?
ECMO is only a “life-sustaining treatment.” It does not cure or treat the disease or injury that led to heart and/or lung failure. This means it is a treatment that can prolong life to allow for more time to try to fix the problem. Sometimes patients do not get better while they are on ECMO because their disease or injury cannot be fixed. A decision about whether there is benefit to continuing ECMO can be hard, and some patients will not want to stay on ECMO if they are not improving. If the healthcare providers believe that the patient’s disease or illness is very severe and will not get better, they will discuss this carefully with the patient and family members and help to make decisions about the end of life and removing the patient from ECMO support. If the patient cannot talk or communicate his or her decision, the healthcare providers will talk with the patient’s legally authorized representative (usually a spouse, parent, or next of kin). While patients can die even though they are connected to ECMO, sometimes ECMO seems to prolong the dying process. It is important to talk to your family members and your healthcare providers about your wishes regarding end of life and what you would like to happen in different situations. The more you clearly explain your values and choices to your loved ones and healthcare providers, the easier they will be able to follow your wishes if and when you are unable to make decisions for yourself. An advanced directive (or a “living will”) is a way to put your wishes in writing to share with others. In the hospital, nurses, doctors, and social workers can provide information about how to complete an advanced directive form.
Extracorporeal Membrane Oxygenation (ECMO)
ECMO stands for extracorporeal membrane oxygenation. The ECMO machine is similar to the heart-lung by-pass machine used in open-heart surgery. It pumps and oxygenates a patient's blood outside the body, allowing the heart and lungs to rest. When you are connected to an ECMO, blood flows through tubing to an artificial lung in the machine that adds oxygen and takes out carbon dioxide; then the blood is warmed to body temperature and pumped back into your body.
There are two types of ECMO. The VA ECMO is connected to both a vein and an artery and is used when there are problems with both the heart and lungs. The VV ECMO is connected to one or more veins, usually near the heart, and is used when the problem is only in the lungs.
USCF is also now using a smaller portable ECMO device that is light enough to be carried by one person and can be transported in an ambulance or helicopter, making it possible to provide ECMO relief in emergency cases.
When is ECMO used:
- For patients recovering from heart failure, or lung failure or heart surgery.
- As a bridge option to further treatment, when doctors want to assess the state of other organs such as the kidneys or brain before performing heart or lung surgery.
- For support during high-risk procedures in the cardiac catheterization lab.
- As a bridge to a heart assist device, such as left ventricular assist device (LVAD).
- As a bridge for patients awaiting lung transplant. The ECMO helps keep tissues well oxygenated, which makes the patient a better candidate for transplant.
Procedure
Being placed on ECMO requires a surgical procedure but it is usually done in a patient's room. The patient is sedated and given pain medication and an anti-coagulant to minimize blood clotting. A surgeon, assisted by an operating room team, inserts the ECMO catheters into either an artery or veins. An x-ray is then taken to ensure the tubes are in the right place. Usually a patient on the ECMO pump will also be on a ventilator, which helps the lungs to heal. While on ECMO, the patient will be monitored by specially trained nurses and respiratory therapists, as well as the surgeon and surgical team. Since you will be sedated and have a breathing tube in place, supplemental nutrition will be provided either intravenously or though a nasal-gastric tube. Nutrition is delivered either intravenously or though a nasal-gastric tube
While on ECMO, you may be given certain medications including: heparin to prevent blood clots; antibiotics to prevent infections; sedatives to minimize movement and improve sleep; diuretics to help the kidney get rid of fluids; electrolytes to maintain the proper balance of salts and sugars; and blood products to replace blood loss. Discontinuing ECMO requires a surgical procedure to remove the tubes. Multiple tests are usually done prior to the discontinuation of ECMO therapy to confirm that your heart and lungs are ready. Once the ECMO cannulas are removed, the vessels will need to be repaired. This can be done either at the bedside or in the operating room. The doctor will use small stitches to close the spot where the tubes were placed. You will be asleep and monitored for this process. Even though you are off the ECMO, you may still need to be on a ventilator.
Risks
ECMO does carry risks including:
- Bleeding, due to the medication that's given to prevent blood from clotting in the tubing.
- Infection at the sites where the tubes enter the body.
- Transfusion problems, since a person on ECMO is given blood products.
- Small clots or air bubbles forming in the tubing.
- Increased chance of stroke.
When does a child need ECMO?
ECMO can help infants and children with a variety of medical problems and conditions, including:
- Meconium aspiration syndrome (MAS): A condition that occurs when meconium, the first stool of a newborn, is inhaled by the baby before or during delivery, and causes lung problems.
- Persistent pulmonary hypertension of the newborn (PPHN): A disorder characterized by abnormally high blood pressure in the arteries that supply blood to the lungs.
- Congenital diaphragmatic hernia (CDH): A condition in which part of the stomach and/or intestines protrude through an opening in the diaphragm into the chest cavity.
- Respiratory distress syndrome (RDS): a lung condition, usually in premature babies, that makes it difficult for babies to breathe on their own.
- Pneumonia
- Congenital heart conditions
- Sepsis
- End-stage cardiac or respiratory failure (as a bridge to transplant)

Our ECMO Core Team consists of approximately ten nurses (RNs) and respiratory therapists (RRTs) specially trained to manage the ECMO circuit. Additionally, there are more than 25 nurses and respiratory therapists trained as bedside ECMO specialists. All CHOP ECMO specialists have a minimum of two years of ICU experience and vigorous training requirements including annual recertification.
There will always be a nurse and an ECMO specialist at your child’s bedside. They will constantly monitor vital signs and comfort, perform care and maintain the ECMO circuit. An “in-house ECMO specialist” is available as a resource to staff 24/7. That person may be the program manager, a Core Team member or a perfusionist (for cardiac cases).
A team of doctors will make rounds (visit the bedside) every morning, assess the progress of your child, and share that information with you. Doctors will also check on your child throughout the day. ECMO patients at CHOP have around-the-clock access to an attending physician through the program’s “ECMO Resource MD” position. In addition, a wide range of specialists are on-call at all times.
What to expect when the child is on ECMO?
Your child will have one or more large plastic tubes, called cannulas, inserted into large blood vessels, most often in the neck. A surgeon places the tubes while your child is under anesthesia. These cannulas provide access directly into the heart and are needed for ECMO to work. Our team will request your consent before performing these operations. Every baby on ECMO receives blood products (we will ask you to sign a consent for this, too).
The blue cannula takes de-oxygenated blood, which has circulated through the body, out of the heart and into the ECMO machine, which adds oxygen to it.
Blood that has been oxygenated by the ECMO machine is pumped into the aorta through the red cannula. The aorta is the large blood vessel that normally carries oxygenated blood out of the heart to the rest of the body.
Even though ECMO does most of the work for the lungs, your child will remain on a breathing machine to deliver controlled amounts of pressure and oxygen to his lungs. The machine also allows the body to get rid of carbon dioxide, usually expelled when you exhale. The breathing tube inserted in the nose or mouth that connects the lungs to the breathing machine is called an endotracheal tube (ET tube).
Your child will also continue to need tubes and lines as she did before receiving ECMO. Most commonly, these include a nasogastric tube, which is placed in the nose and guided into the stomach to decompress and keep the stomach empty of acid; intravenous lines to provide fluids and medications; and a tube into your baby’s bladder to drain urine. Your child may also have a chest tube placed into the chest through the chest wall to drain air or fluid outside the lungs.
Your child will receive medication to treat any pain or discomfort while on ECMO. Pain medication is usually given as a continuous infusion into the ECMO circuit. Other medications frequently given during ECMO include diuretics to help your child urinate.
Swelling, also known as edema, is an expected side effect of ECMO. The medical staff caring for your child will monitor the condition closely.
While on ECMO, your child may undergo a variety of tests to monitor her condition, including:
- Blood gases (such as an arterial blood gas, or ABG) to monitor the oxygen and carbon dioxide levels in the blood.
- Complete blood count (CBC): This test monitors levels of red and white blood cells and platelets (cells in the blood that help to form blood clots) and tells us if we need to transfuse your baby with blood products.
- Basic metabolic panel (BMP): These tests monitor electrolytes (including calcium, potassium and other substances), which are needed in a certain balance for the body’s systems to run. These tests tell us which electrolytes we need to give your baby through the IV lines to keep them at normal levels. The BMP also helps us monitor kidney function, which is very important to your baby’s health.
- Tests to check your baby’s blood so we can adjust anticoagulant medications (“blood thinners” such as Heparin) during ECMO support and hemoglobin/hematocrit levels in the blood.
- Imaging tests done at bedside to monitor your baby’s progress, including X-rays to check the location of the cannulas and monitor inflation of the lungs; ultrasound of the head to monitor for complications related to bleeding; electroencephalogram (EEG) to monitor brain activity: and echocardiogram (an ultrasound of the heart) to assess how the heart is doing as we attempt to wean your baby from ECMO support.
Your child will be given sedation medications to keep her from moving around. This is necessary to keep the ECMO circuit in place and working correctly. The sedation medications will make your child sleep most of the time. Even though your child is sleeping, you can still talk to and carefully touch your child. Because it is important to let your baby rest while on ECMO, the ECMO specialist can guide you when it is safe for your baby to be stimulated.
Children, including infants, can hear and recognize the sound of their parents’ voices while sedated. Your child (and you) may find it comforting if you talk to him or hold her hand gently. Ask a child life specialist or other staff member for ideas on how to interact with your child.
The equipment being used to treat your child is quite delicate, so it is very important that you do not touch the cannulas, the machinery or the settings. For this reason, you won’t be able to hold your child while she is on ECMO. Keep a safe distance from the circuit, so you don’t accidentally bump into it. If you have questions about the equipment, please feel free to ask the ECMO specialist on duty who is caring for your child.
Your child will come off of ECMO when the heart and lungs have recovered enough to function without the ECMO circuit. This can take several days or several weeks, and it depends on your child’s specific diagnosis and course of treatment. As daily test results begin to show progress, the care team may slowly lower settings on the circuit to allow your child’s body to gradually function on its own, at which time the cannulas will be surgically removed.
After ECMO
Immediately following removal of the cannulas and ECMO circuit, your child will need to remain on a ventilator to maintain oxygenation. Nitric oxide is a gas given through the ventilator to relax blood vessels. Over time, the goal is to wean your child slowly from the ventilator and medications. A nurse will continue to closely monitor vital signs and signs of pain and perform ordered lab work. While each child is different, be prepared that your child’s recovery period from ECMO may be measured in weeks and months, rather than days.
Advise to Parents whose child is on ECMO
Having a child on ECMO can be emotional, even traumatic, for parents, guardians and family. You will likely find that the experience is filled with many ups and downs. The following is advice from other parents who have been in your shoes.
- First and foremost, take care of yourself. Eat, sleep and get outside every day. You will need to make decisions about your child’s medical care, which you can do only if you are rested and alert.
- Be an active participant in your child’s care. Most parents have no medical training and find it difficult to understand much of the medical terminology and information. Ask questions to help you understand what is happening and to help you make decisions. The Hospital staff will make every attempt to answer all your questions.
- Use Hospital resources. There are many resources available at CHOP, free of charge, that may make your time less stressful. These include: sleep rooms (when available), a reference library, laundry, computers with Internet access, emotional counseling and more. Ask your bedside nurse for information.
- Talk to a Hospital social worker, who can help ease your stress by talking about issues that concern you.

Cost of ECMO in the United States
n average ECMO procedure costs 73,122 USD and that an average ECMO patient had a total hospital cost of 210,142 USD – demonstrate that ECMO is a highly resource-demanding procedure. The major portion of the costs is related to treatment in the intensive care unit (ICU)

Outcome of inter-hospital transfer of patients on extracorporeal membrane oxygenation in Europe.
Abstract
AIMS OF THE STUDY:
An extracorporeal membrane oxygenation system (ECMO), as a bridge to either recovery, a ventricular assist device (VAD), or heart or lung transplantation, may be the only lifesaving option for critically ill patients suffering from refractory cardiac, respiratory or combined cardiopulmonary failure. As peripheral hospitals may not offer ECMO treatment, tertiary care centres provide specialised ECMO teams for on-site implantation and subsequent patient transfer on ECMO to the tertiary hospital. This study reports the results of the largest ECMO transportation programme in Switzerland and describes its feasibility and safety.
METHODS:
Patients transported on ECMO by our mobile ECMO team to our tertiary centre between 1 September 2009 and 31 December, 2016 underwent retrospective analysis. Implantation was performed by our specialised ECMO team (primary transport) or by the medical staff of the referring hospital (secondary transport) with subsequent transfer to our institution. Type of ECMO, transport data, patient baseline characteristics, operative variables and postoperative outcomes including complications and mortality were collected from medical records.
RESULTS:
Fifty-eight patients were included (three patients excluded: one repatriation, two with incomplete medical records). Thirty-five patients (60%) received veno-venous, 22 (38%) veno-arterial and one patient (2%) veno-venoarterial ECMO. Forty-nine (84%) patients underwent primary and nine (16%) secondary transport. Thirty-five (60%) patients were transferred by helicopter and 23 (40%) by ambulance, with median distances of 38.1 (13–225) km and 21 (3-71) km respectively. No clinical or technical complications occurred during transportation. During hospitalisation, three patients had ECMO-associated complications (two compartment syndrome of lower limb, one haemothorax after central ECMO upgrade). Median days on ECMO was 8 (<1–49) and median days in hospital was 17 (<1–122). ECMO weaning was successful in 41 patients (71%), on-transport survival was 100%, 40 patients survived to discharge (69%), and overall survival was 67% (39 patients) at a median follow-up of 58 days (<1–1441). Cumulative survival was significantly affected by cardiogenic shock vs. ARDS (p = 0.001), veno-arterial and veno-venoarterial vs. veno-venous ECMO (p = 0.001) and after secondary vs. primary transport (p <0.001). The ECMO weaning rate was significantly lower after secondary transfer (22%, two patients, both vaECMO) vs. primary transfer (80%, p = 0.002, 39 patients of which 35 (71%) had vvECMO).
CONCLUSIONS:
The first results of our ECMO transportation programme show its feasibility, safety and efficacy without on-site implant or on-transport complications or mortality. The favourable early survival may justify the large effort with respect to logistics, costs and manpower. With rising awareness, referring centres may increasingly consider this lifesaving option at an early stage, which may further improve outcomes.
About New York
Location of New York:
Latitude: 40.6943Longitude: -73.9249
Details of Airport Indianola Municipal Airport in New York :
IATA:ICAO:
Latitude: 33.485699
Longitude: -90.678902
Altitude: 126
Time (UTC): -6
DST: A
Timezone: America/Chicago
Country: United States
About Mumbai
Location of Mumbai:
Latitude: 19.017Longitude: 72.857
Details of Airport Chhatrapati Shivaji International Airport in Mumbai :
IATA: BOMICAO: BOM
Latitude: 19.08869934
Longitude: 72.86789703
Altitude: 39
Time (UTC): 6
DST: N
Timezone: Asia/Calcutta
Country: India
Mumbai (formerly called Bombay) is a densely populated city on India’s west coast. A financial center, it's India's largest city. On the Mumbai Harbour waterfront stands the iconic Gateway of India stone arch, built by the British Raj in 1924. Offshore, nearby Elephanta Island holds ancient cave temples dedicated to the Hindu god Shiva. The city's also famous as the heart of the Bollywood film industry.
Mumbai is a tertiary care center and receive patients from North East and South India for advanced Treatment to all major tertiary care centers.
Advanced Eye Hospital and Institute
Asian Heart Institute
B
B.D. Petit Parsee General Hospital
Bhabha Hospital
Bhaktivedanta Hospital
Bombay Hospital
Breach Candy Hospital
C
Cama Hospital
Cooper Hospital
Currae Hospital
G
Gokuldas Tejpal Hospital
H
Holy Family Hospital, Mumbai
Holy Spirit Hospital (Mumbai)
Hurkisondas Hospital
J
Jaslok Hospital
JJ Hospital
K
KEM Hospital
Kokilaben Dhirubhai Ambani Hospital
L
Lilavati Hospital and Research Centre
Lokmanya Tilak Municipal General Hospital
M
Masina Hospital
N
Nanavati hospital
P
P.D. Hinduja National Hospital and Medical Research Centre
Parsi Lying-in Hospital
Prince Aly Khan Hospital
R
Rajawadi Hospital
S
Saifee Hospital
St George Hospital, Mumbai
SevenHills Hospital
Shroff Eye Hospital
Shushrusha Citizens' Co-operative Hospital
T
Tata Memorial Centre
U
Umrao Hospitals

The Gateway of India is, without doubt, one of the most popular tourist hotspots of Mumbai. Sitting proudly on the Apollo Bunder, it overlooks the Arabian Sea. It is one of the defining monuments of the city of Mumbai and was built in the year 1924. The construction was undertaken by the famous architect George Wittet, to commemorate the visit of King George V and Queen Mary to Mumbai. The imposing structure of the monument is a beautiful confluence of Indian, Arabic and Western architecture and has become a popular tourist hub in the city. It is also the starting point of a number of ferry services that ply to the historic Elephanta Caves.
Nicknamed 'Mumbai's Taj Mahal', the foundation of this landmark was laid in 1911 and it was inaugurated 13 years later in 1924. The structure in itself is a made of yellow basalt and solid concrete and is embellished with numerous Muslim and Hindu motifs as well. The basalt arch of the Gateway served as the entry and exit access to India through waterways before independence and was the exit point from where the last British ship left India for England. There are statues of Swami Vivekananda and Chhatrapati Shivaji that have been installed near the Gateway as well. The view from the sea of the Gateway complex, especially at night is quite ethereal and beautiful. The Gateway of India is thus, not only a historic artefact but an example of marvellous architecture in itself!
History of Gateway of India
The land on which the Gateway now stands once belonged to a jetty that was primarily used by the fishing community of the area. Seeing its viability as a landing area, it was renovated to serve as a pier for British governors. Soon enough, it was decided that a grand gateway will be built here to welcome King George V and Queen Mary to Mumbai, and the foundation of the same was laid down March 31, 1913, by the Governor of Bombay, Sir George Sydenham Clarke. However, the final design of the Gateway was only sanctioned on March 31, 1914, by George Wittet. The constructions formally began in 1920 and it took almost four years to complete the construction of the monument.
Built in Indo Saracenic style, the Gateway of India was designed by Scottish architect George Wittet. The design is a combination of Hindu and Muslim architectural influences along with a Roman triumphal arch, which stands at a height of 26 metres. It is built of yellow basalt and concrete and the stone was sourced locally. The arch is flanked by two large hallways that have the capacity to accommodate as many as 600 people. On the other hand, the central dome of the gateway is inspired from Muslim architecture style and has a diameter of 48 feet with the apex reaching 83 feet. The gateway also has meticulously designed honeycomb structures which further support four spires that grant a unique symmetry to the facade. Steps behind the archway give an expansive view of the Arabian Sea as well.

Prince of Wales museum, Mumbai Overview
The Prince of Wales Museum is a splendid structure situated in Mumbai and is regarded to be one of the heritage buildings of the city. The foundation stone of this edifice was laid down by the Prince of Wales on the 11 November 1905, and it was established as a museum on 10 January 1922. The facade of the museum is a sight to behold in itself and sits in the midst of an expansive green garden. Adorned with stunning stone and lattice work, the architecture of the Prince of Wales Museum is a blend of Indian, Mughal and British engineering styles. Inside, the museum holds almost 50,000 of some of the most exquisite artefacts relating to the rich and diverse history of India.
Now known as 'Chhatrapati Shivaji Maharaj Vastu Sangrahalay', The Prince of Wales Museum is a Grade I Heritage Building of the city and is counted amongst one of the most prominent museums of India. The complex exhibits a myriad collection of ancient artefacts, artwork and sculptors of the country which give a unique insight into our past. The building also underwent a major renovation after which several new galleries adorning the artworks of Hindu God Krishna, textiles and Indian traditional costumes were opened. Preserved in its best form, the Prince of Wales Museum is a wonderful manifestation of India's glory and rich past.
National gallery of Modern Art, Mumbai Overview
A paradise for art lovers, National Gallery of Modern Art (NGMA), Mumbai is a famous art museum possessing a magnificent collection of paintings, sculptures and artefacts since 1996. The multitude of artwork present in this charismatic gallery has drawn millions of visitors and left them awestruck. It is governed by the Department of Culture, Government of India and has over the period become a popular tourist attraction as it very convincingly depicts the modification of artwork in the field of visual and plastic arts. A blend of art and culture, this gallery houses the artworks of phenomenal sculptors, artists and painters including the legendary Pablo Picasso who is considered as the epitome of art and painting. The oldest artwork is known to be around 160 years old. The ancient artefacts such as statues and mummies from Egypt have also a played a crucial role in rousing the curiosity of the visitors.
The National Gallery of Modern Art also organises various art exhibitions which provide an intriguing platform to both the artists and the art lovers as the artists get a remarkable opportunity to showcase their talent while the art lovers can explore and quench their thirst for art. The gallery is located near Regal Cinemas in Colaba, South Mumbai. It showcases some of the oldest artworks, dating back to 1857 and is considered one of the best in India.

Haji Ali Dargah, Mumbai Overview
Situated on the backdrop of a beautiful view of the Arabian sea is the shrine of Haji Ali, dedicated to the wealthy merchant turned who gave up his worldly belongings and turned into Muslim Sufi saint after a trip to Mecca. Haji Ali Dargah is located on a small islet that is off the southern coast of Mumbai near Worli. People from all walks of life and religions come here to seek blessings. The Dargah can only be accessed during the low tides via a causeway that is surrounded by the sea on all sides. At night, the view of the shrine lit up in the distance with nothing but the sea around it, is a divine sight.
Built of glass, the tomb is a beautiful illustration of the Indo-Islamic style of architecture. A marble courtyard contains the central shrine. The tomb within the mosque is roofed by a brocaded red and green cloth, supported by an exquisite silver frame and marble columns. The main hall has marble pillars engraved with creative mirror work: blue, green, yellow chips of glass arranged in varied designs and Arabic patterns which spell the ninety-nine names of Allah. As per Islamic customs, there are different praying rooms for ladies and gents.
Haji Ali belonged to Bukhara, which lies in present-day Uzbekistan. This shrine has a mystical story attached to it. According to legends, Sayyed Peer Haji Ali Bukhari once came across a poor woman crying on the road and holding an empty vessel. Upon inquiring about the matter, she told him that she had spilled the oil she was supposed to be carrying home and was now afraid that her husband will punish her. He then accompanied her to the spot where she had spilled the oil and prodded the ground and oil came gushing out. The woman was delighted and went home happily. Later, recurrent dreams indicating that he had injured the Earth haunted him and his health began to deteriorate. He then decided to travel to India and decided to stay here so as to spread the word of Allah and Islam.
From that point of time till the end of his life, Haji Ali dedicated his life spreading the wisdom of Allah and devotees would regularly visit him. Before he died, he instructed his followers that they shouldn't bury him immediately, rather they should drop his shroud in the ocean and bury him where it is found. In accordance with his wishes, the Haji Ali Dargah was built in the year 1431. According to another belief, Haji Ali donated all his wealth for a journey to Mecca and died in between. Miraculously, the casket carrying his body floated back to Arabian shores and got stuck in the twine of rocky islets just off the shores of Worli.

The Siddhivinayak Temple in the Prabhadevi area is a revered shrine dedicated to Lord Ganesha and is one of the most significant and frequented temples in Mumbai. This temple was built in the year 1801 by Laxman Vithu and Deubai Patil. The couple did not have any children of their own and decided to build the Siddhivinayak temple so as to fulfil the wishes of other infertile women. Interestingly, the statue of Lord Ganesha here is believed to be self-manifested and grants wishes.
The Temple has a small sanctum housing the idol of Shri Ganesha, which is about two and a half feet wide and made out of a single piece of black stone. The temple has attained a popular status not only because it is believed that the Ganesha in the temple is especially revered, but also because of its popularity with Film stars and the bigwigs of the industry. It is also the richest temple in Mumbai as it begets INR 100 Million in donations each year from devotees across the world.
The story behind the construction of the Siddhivinayak temple is that of faith and belief in the Lord. The building was funded by rich Agri woman named Deubai Patil, who did not have any children of her own. She decided upon building a temple dedicated to Lord Ganesha so that he may fulfil the wishes of other childless couples and bless them with children. The construction of the Siddhivinayak temple was completed on 19 November 1801, with the original structure being a square edifice adorned with a dome - shaped spire. Ramakrishna Jambhekar Maharaj who a disciple of the Hindu saint Akkalkot Swami Samarth, buried two idols in front of the present idol upon the instructions of the Swami. As was prophesied by Swami Samarth, a Mandar tree sprouted from the buried idols with the image of Svayambhu Ganesha in its branches after a period of 21 years.
The imposing structure of Shree Siddhivinayak temple comprises of a primary 'Kalash' which towers to a height of 12 feet, three reaching up to 5 feet and 33 others which stand at a height of 3.5 feet. Thus, 37 gilded domes embellish the main temple complex. The old part of the Siddhivinayak temple has a hall, the main sanctum, a verandah and a water tank as well. The new complex of the temple was built as a part of renovations so as to enhance the magnificence of this shrine. The architect Ar. Shri. Sharad Athale of SK Athale & Associates made a study of the temples in Rajasthan and Tamil Nadu before finalising the design of the temple. After making the necessary arrangements, the construction of the Siddhivinayak temple commenced in the year 1990. The old idol was kept intact whilst a multi angular six - storey structure was built over the gold plated domes. Three main entrances leading up to the interior were constructed and the crown of the temple was redesigned as well. After meticulous work that was spread over a timeframe of three years, the construction gave way to the Siddhivinayak temple as we know it today.
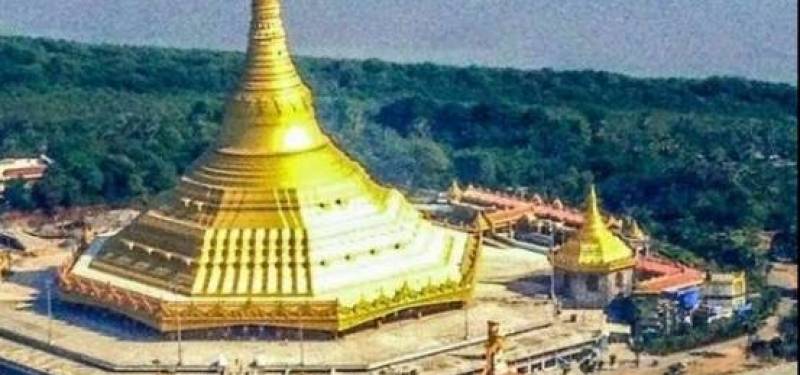
Global Vipassana Pagoda, Mumbai Overview
It is tough to imagine that one of the quietest and most peaceful spaces can exist right in the middle of the busy suburbs of Gorai in Mumbai. The Global Vipassana Pagoda is a meditation hall shaped like a dome with a capacity to seat of 8,000 devotees and Vipassana practitioners. Along with admiring the serenely mesmerizing Pagoda located on a peninsula between Gorai creek and the Arabian Sea. Another interesting facet of the monument is that it has been completely through donations. Visitors can take a short 10-minute Aanapana Meditation session to experience how invaluable the technique of meditation is and then decide if they want to enrol for a long term course. No matter what the verdict is, a trip to the Global Pagoda will be worthwhile.
The Global Vipassana Pagoda was built as a token of gratitude towards a Vipassana teacher and Accountant General of Independent Burma, Sayagyi U Ba Khin, who was instrumental in bringing Vipassana back to its country of origin after it ceased to exist in India. Many visitors frequent the Global Pagoda during the stressful and painful phases of their lives and manage to achieve total harmony in the chaotic times of today. It is also considered to one of the seven wonders of the state of Maharashtra.
The Global Pagoda's planning began in 1997, but the actual construction started only in 2000. The idea of constructing a Global Pagoda was proposed by Shree S.N.Goenka, to spread the true teachings of Lord Buddha. Over the years, religious dogmas prevailed, and the correct path of Dhamma was forgotten. These lessons had to be instilled again in the minds of people who were blinded by the religious dogmas and the introduction to an improved way of life was required to increase tolerance and maintain peace and harmony in the world.
Acharya Goenkaji firmly believed that the Pagoda would serve as a helpful vehicle to spread the true meaning of Dhamma and inculcate the age-old technique of Vipassana that ceased to exist nearly two million years ago. For the exemplary work put in by Acharya Goenkaji, he was awarded the title of Padma Bhushan in the year 2012 on the occasion of Republic Day. A little over a year later, on 6th June 2013, the Global Pagoda was included in the list of the Seven Wonders of Maharashtra for its development, architecture and purpose.
The Global Vipassana Pagoda has been constructed on 13 acres of land and is an illustration of the traditional Buddhist architecture with traditional Burmese designs. The Burmese designs have been included in the structure as a sign of respect and gratitude towards Myanmar for preserving the practice of Vipassana Meditation. The dome-shaped pagoda is a combination of ancient and modern Indian technology, and its shape is a replica of the Shwedagon Pagoda (Golden Pagoda), Myanmar, which makes the structure strong enough to stay put for at least a thousand years.
The entire structure is covered in gold coloured paint, and the spire or the shikhara of the pagoda is covered in real gold that was donated by the Burmese. The spire is topped with a decorative piece that resembles an umbrella. The humongous inner dome enables 8000 people to practice Vipassana meditation together at one time. The entrance doors are made of wood that has been hand-carved intricately in Myanmar.
The foundation of the structure is made of Basalt rocks, and the dome is made from sandstone that was brought from Rajasthan. Each sandstone block weighs around 600 to 700 kilograms and is secured in place with the help of bricks designed to interlock. These uniquely designed bricks and lime mortar hold the sandstone in place and help the structure stand for several years. The large pillar-less dome, in the centre, has a height of 29 meters. The entire structure of the pagoda is 96.12 meters tall. The interior of the pagoda is hollow and serves the purpose of a huge meditation hall; which covers an area of 6000 square metres. The top of the pagoda is completed with a large crystal.
Beginner Course: The beginner course is a 10-day course during which they have to follow the course rules and regulations that include adhering to the timetable, not harming any living being, no sexual misconduct, no lies and no consumption of intoxicants. The students practice ten hours of meditation every day (includes regular breaks). The first three days are to develop concentration through Aanapana and the next seven days are for complete Vipassana Practice. On the last day, the Metta Bhavana technique of meditation is taught and practised. These courses are bilingual and can be attended by participants who do not understand regional languages.
10-day Executive Course: These courses are introductory courses planned especially for Business Executives, Entrepreneurs and Government Officials
Old Students Short-term Course: The participants who have completed at least one 10-day program are considered as old students. They can enrol for a 3-day short course each year to stay updated with the technique.
Advanced Courses: This includes the same timetable as that for the beginner courses, however, the duration and the intensity of meditation is a little more advanced. Participants can choose between 20, 30, 45 and 60 days of course periods.














